THE ROLE OF PHYTOTHERAPY IN CONVENTIONAL CANCER TREATMENT.
On the base biomedical properties and computerized analyses of traditional and non-traditional plants we determine the effectiveness of action of medical plants to the symptoms, syndromes and different kind of oncological diseases in general. The best results in the treatment of oncological patients we reached with usage of necessarily surgery, with accompany chemotherapy and radiation therapy and with combination of phytotherapy. Treatment by this schema with usage of our new formulas enhanced the average of survivals the first year after treatment from 39% (official data of Russian Health Ministry) to 90%, in our case. More than 50% of our patient treated by this way lived more than 5 years. According to our new approach cancer is chronic disease, with weakness of immune system. So, it should be treated as a chronic disease with monitoring of immune system. To be sure that recurrence of malignant is not appears any more it was created special formula, which can be used during the whole lifetime.
The aim of cancer therapy is the destruction of the tumor and to preserve function and lengthen survival time. The main therapies are surgery, chemotherapy and radiotherapy. However, they may negatively impact quality of life. Because only maximum dosages can eliminate all malignant cells and cytotoxic substances not only damage the tumor cells, they also affect all other bodily systems. Medical Plants can help minimize side effect of conventional treatment. Recent studies demonstrate that, even after maximum therapy (surgery, radiation, and chemotherapy) still about 0.1% of rest tumor cells have survived (Joachim Fluhrer 1995). Only the immune system is then capable of achieving a cure. Usually immune system can destroy these remaining malignant cells, but the tumor-destructive therapies have damaged the immune system quite extensively. Therefore a high risk of recurrence and metastases will exist. Phytotherapy can be used to optimize the endocrinological therapy and stimulate the immune system. During phytotherapy a supportive therapy for liver function and the micronutrient balance is essential. Phytotherapy can be employed as an effective method in the treatment of digestive tract cancer allowing us to individualize therapy accordind to immunologic, endocrine and metabolic characteristics of the patients (S.I.Yalkut, et al.-2000). All immunologic effective substances need to be considered such as the vitamins, phytochemicals, such as
*Corresponding author: Dr. Danik M. Martirosyan, D&A Inc., Richardson, TX, USA, E-mail: danikm@sbcglobal.net
anthocyanosides, phenolic acids, flavonoids, coumarins, poly-acetylenes and carotenoids. This article explores the role of Phytotherapy for improving the quality of life, and perhaps survival time, of oncological patients.
For the treatment of oncological diseases we used medical plants by the fallowing way:
Dry botanical collections (Species);
Could infusions (Infusum);
Hot infusions (Infusum);
Decoctions (Decoctum);
Unguents (Unguentum);
Pills from dry herbs with special extenders (Tabulettae);
Phytochitodeses made on the base of chitosan and botanical collections.
All this materials was made by special methods described by Dr. Treskunov K.A. in the book of “Memoirs of Phytotherapist” – 12003, Moscow, pp 205—208.
Treatment was provided with monitoring of syndromes, symptoms and immune system. Monitoring of immune system we reach by investigations of formal elements of blood system, in particularly trombocytes, leucocytes, erythrocytes and CEO. Monitoring of syndromes and symptoms was provided by investigations of Ache, Itch, Icterus, Nausea, Diarrhea, Constipation, Decrease of appetite, Cough, Wheeze, Exhaustion, Weakness, Depression, Dizziness, Headache, Edema, Ague, Bleeding, Extravasations, Canker, erosions and Anemia.
First step of treatment of oncological patients with herbal plants we start 2-3 days before surgery, chemotherapy and radiation. Our formula (number 02), which is used in the step 1 contain Chamomile, Goose Grass, Mint, Tutsan and Milfoil. Patients can used that as a pill or as a capsule. There are not side effects from those and at present time they are proved from Russian Ministry of Health Ministry. This formula mainly we using for the stimulation of immune system and to preventing the side effects of chemical and radiation therapy.
Second step is prevent and treatment of the side effects of chemotherapy and radiation. After conventional treatments often have been observed anemia, leykopenia, trombocitopenia. In this step we are using formula number 05, which contain more than 20 plants. Patients using this formula as a tablets 3-4 times a day within 10-12 days until immune and blood system renewal.
Third step is usage of formula number 01. This one oncological patient have to use during the hole life time, without any brake more than 1 month, to be sure that recurrence is not appears any more.
It was investigated 4 groups of oncological patients. First group content 150 patient which is 33% from total amount of oncological patient to whom was provided phytotherapy with surgery, chemotherapy and (or) Radiation. The second group composed of 92 people, which is 20% of total patients. They get surgery additional to the phytotherapy.
The third grope was 127 patient (28% from total amount) who get phytotherapy, chemotherapy and (or) radiation, without surgery. Forth group composed of 82 patients, which is 19% of total amount. They were treated with only phytotherapy.
Our data shown that the treatment with phytotherapy jointly with surgery, radiation and chemotherapy provide the best results (group 1 and group 2). It is interesting that 21% survivors of oncological patients treated only with phytotherapy, without any conventional healing live more than 5 years. It was shown also that in the case of combination of surgery, chemotherapy, and radiation with phytotherapy there is no complication, which is usually having a place without herbal healing. We find out also, that the usage of our formulas as a tea lifelong prevents beginning of recurrences.
It is well known, that each year in Russia apiaries more than 400 000 oncological patients. From thous 39% only usually live more than 1 year. Thus we contributed a new approach for treatment of oncological diseases. The new approach considering condition of immune system of patient before and after conventional cure. It is known that Immune system become a week after radiation and chemotherapy.
As a pioneer we receive a authentic statistics which proved effectiveness of phytotherapy in general and effectiveness of each herbal plant in particular, which we using in depends of syndromes and symptoms, illness, etiology and pathogenesis. On the base of computerized analyses we find out the effectiveness’s of action of medical plants to the symptoms, syndromes and diseases. Thus we determine that the most effective among the investigated plants as an anesthetic is “air bolotniy”, then “shalfey lekarstvenniy”, and tarragon at cetera. This is very important because in the case of oncological diseases usually appears strong pain, which is only you can decrease with anesthetics. Furthermore we find out that in the case of weight lose the best medical plant are “xvoshch polevoy”, nettle, coltsfoot, mint and chamomile. This allows as composing most effective phyto collection for each individual patient. With the usage of phytotherapy in our case disappears or vastly decreases pain, renew of leucocytes (78%) vomit (75%), thrombocytes (80%), hemoglobin – 65%, renew weight of body (70%), disappears depression (77%) and weakness (77%). The usage of chemotherapy and radiation jointly with phytotherapy prevents the development of chemical or X-ray illness.
Numerous published protocols confirm the importance of nutrition’s and herbal therapy in speeding post-surgical healing and reducing pain, swelling, and complications (Wright TV, 1996; White LB, 1998). Supplement protocols begun 1-2 weeks prior and continuing 3-4 weeks post-surgery-commonly include a daily intake of Vitamin C (3,000 mg), Bioflavonoids (1,500 mg), Vitamin E (400 IU), Vitamin A (25,000 IU), and Zinc (30 mg). Proteolytic enzymes--well researched in cancer treatment are particularly helpful in reducing swelling and enhancing wound healing.
Our results confirm that the usage of phytotherapy in our case vastly decreases pain, weakness and anemia but its also lead to the renew of leucocytes (78%), thrombocytes (80%), hemoglobin – 65%. This is can prove our hypothesis, that phytotherapy can be directly involved in the renewal of weak immune system of oncological patient.
There is a strong connection between tumor genesis and immunological “weakness”. With the knowledge we have today about this connection, no oncological therapy should be done without immunological control. After the diagnosis of cancer, the damaged cellular defense mechanism has to be treated and restored as early as possible. Consequent immune monitoring and specific immune modulation increases the chances of successful therapy. Many substances with immunological effect have a high degree of importance in the supportive cancer therapy of any cancer patient. It is well known that macrophages, NK-cells, cytotoxic cells and helper cells can attack malignant cells and destroy them (Hager E.D. 1994). At the time of diagnosis, and even before, one usually finds a very low cellular immunity. Tumor-associated antibodies produce immunocomplexes, together with the corresponding antigens. Above a certain concentration, macrophages are not able to destroy those immunocomplexes any more (Joachim Fluhrer, 1995). These complexes will then build a barrier around the tumor and therefore prevent an active immunological reaction against tumor cells. In higher concentration, circulating immunocomplexes block the function of macrophages and so paralyze an important defense mechanism. A healthy defense and immune system can identify and destroy cancerogenic substances and disease will not ensue. If the limit of the compensatory ability of the immune system is reached, or if there is a cellular immunodeficiency, then penetration of the cancerogenic substances into the basal membrane or the cell membrane can occur (Tullberg Th., 1979). Interaction with nuclear DNA will lead to the formation of oncogenes and oncogenic cells. Tumor antigens can stimulate the production of specific antibodies, which are directed against specific cell structures. If the immune system is still intact the 'malignant' process can still be interrupted and total restoration is possible. If the cellular immune system is too weak, uncontrolled growth of tumor cells can occur, either encapsulated or invasive. The encapsulated tumor can be removed surgically and a cure is possible. If the cancer has invaded the blood vessels or lymphatic system, then malignant cells have become systemic. Even then the immune system has the possibility to identify and destroy the malignant cells and prevent the progression of the disease (Joachim Fluhrer, 1995. In our case phytotherapy at this stage is still effective (21%), but it is mach better if it is provided with surgery and other forms of conventional treatment (51%). If treatment of cancer with phytotherapy jointly surgery is missed, then the 'malignancy' has escaped the control of the immune system and will lead to the death of the patient.
Monitoring the immune system at the time of diagnosis and then regularly afterwards is of extreme importance. In the first 2 years following the diagnosis and treatment of cancer, a 6-weekly monitoring of the immune status should be done, especially if immune-modulator therapies are being used. After stabilization less frequent monitoring is necessary. It should be monitored the fallowing cells of immune system: T-Lymphocytes, suppressor cells, helper cells, Macrophages, B-lymphocytes, leucocytes, thrombocytes, hemoglobin.
Immune Modulation in Cancer Therapy can be provided as well as with phytotherapy and with Phytochemicals, including Quercetin and Rutin, Micronutrients, such as Zinc, Magnesium, Selenium, Lithium, with vitamins such as Vitamin A, Beta-Carotene, Vitamin C, Vitamins B2, B6, B12 and Folic Acid.
In the case of Immune therapy may activate sub clinical infections (e.g. silent dental abscesses, ostitis, impacted wisdom teeth, etc.) and therefore enhance the biological stress. This may lead to a worsening of the immunological status. Usually herbal therapy has not side effect, so we suggesting provide phytotherapy with monitoring immune system. Only after effective therapy will the cellular immune defense rise again. To enhance the efficacy of Radiation Therapy we provided phytotherapy with the fallowing plants:
We believed that these plants supplied the body with necessary phytochemicals and nutrients also. Usually, enhancing the efficacy of Radiation Therapy provided with niacin, Anti-oxidants, Vitamin C, and Vitamin E. Oxygen is a potent radiation sensitizer. Hypoxic (oxygen-deficient) tumors are resistant to radiation. Natural agents that increase blood flow may improve radiation response by delivering oxygen to tumors, thereby increasing tumor vulnerability to radiation. Niacin (500 mg to 6,000 mg of nicotinamide) is an effective radio-sensitizer, while producing little or no radio-sensitization of normal tissues.13-17 however, prolonged intake of larger doses of niacin may lead to liver damage. Inositol hexaniacinate may be a preferable form. It is safer, well tolerated, and effectively improves circulation and oxygenation.18 Radiotherapies are believed to achieve their cytotoxic effect by generating free radical-mediated DNA damage to the tumor. The use of anti-oxidants during radiation therapy appears counter-indicated in theory. However, research published over the past 30 years supports the adjunctive use of anti-oxidant nutrients, with improved radiation treatment results and protection of healthy tissues (Cheraskin E, et al-1968; Funegard U, et al., 1995; Stahelin HB, 1993; Wood U, 1985; Wadleigh RG, et al-. 1992; Lissoni P, et al. 1997).
Vitamin C Increases tolerance to radiation therapy without reducing tumor control (Okunieff P, et al-1991). Vitamin E is also an effective adjunct to radiation (Prasad KN, 1993; Myers C.E., et al.1982). It protects against brain edema (Yoshida S, et al-.1992), a side effect of brain irradiation. Vitamin E intake (800 IU/day) can be divided between d-alpha tocopheryl succinate, which does not act as an anti-oxidant and provides some anti-tumor effects, and a mixed tocopherol product.
Side effects of Radiation Therapy commonly associated with brain irradiation include loss of hair, skin burn, loss of taste, and pervasive fatigue. Radiation damage to salivary glands and taste buds can result in a dry, irritated mouth and loss of taste perception. This can decrease the desire and ability to eat, seriously impacting nutritional status. Post RT healing can be provided with zinc, flaxseeds, Topical vitamin E, Aloe Vera and Ginseng. Zinc supplementation (15-45 mg, as lozenges or liquid zinc sulfate) at onset of loss of taste can restore taste perception (Ripamonti C, et al.1998). Supplementation with antioxidant nutrients--from 14 days prior through 12 days post-RT---can reduce damage to salivary glands (Funegard U, et al., 1995) Water extracts of flaxseed can provide relief of dry, irritated mouth and replace lost saliva (Andersson G, et al, 1995). Topical vitamin E is effective in oral mucositis (Wadleigh RG, et al, 1992). Topical application of 100% concentrate of Aloe Vera after daily RT treatments can be helpful for radiodermatitis. Vitamin E supplementation (1,600 IU/day), begun one week prior to RT, allowed more than half the patients to keep their hair, and dramatically reduced fatigue. Ginseng is best restricted to recuperation following RT (15-30 days post-RT), because it stimulates DNA rep
Further studies are needed in the specific effect on cancer cells. From our investigations we can make the fallowing conclusions:
1. On the base biomedical properties and computerized analyses of traditional and non-traditional plants we find out the effectiveness of action of medical plants to the symptoms, syndromes and different kind of oncological diseases.
2. It was created new formulas, which are enhancing the damaged cellular defense mechanism of oncological patients. They prevent the beginning of side effects of chemotherapy and radiation therapy and healing the side effects of conventional therapy. There are not side effects from these formulas, they are cast effective and at present time they are proved from Russian Ministry of Health Ministry.
3. The best results in the treatment of oncological patients we reached with usage of necessarily surgery, with accompany chemotherapy and radiation therapy and with combination of phytotherapy. Treatment by this schema with usage of our new formulas enhanced the average of survivals the first year after treatment from 39% (official data of Russian Health Ministry) to 90%, in our case. More than 50% of our patient treated by this way lived more than 5 years.
4. According to our new approach cancer is chronic disease, with weakness of immune system. So, it should be treated as a chronic disease with monitoring of immune system each 6 month. To be sure that recurrence of malignant is not appears any more it was created special formula, which can be used during the whole lifetime.
2. Brown JM, et al. Structure-activity relationships for turnour radio-sensitization by analogues of nicotinamide and benzamide. Int J Radiat Biol 59(3): 739-748, March 1991.
3. Cheraskin E, et al. Effect of diet upon radiation response in cervical carcinoma of the uterus: a preliminary report. Acta Cytol 12(6): 433, November/December 1968.
4. Funegard U, et al. Can alpha-tocopherof and beta-carotene supplementation reduce adverse radiation effects on salivary glands? Europ J Cancer 31A(13-14): 2347-2353, December 1995.
5. Funegard U, et al. Can alpha-tocopherol and beta-carotene supplementation reduce adverse radiation effects on salivary glands? Europ J Cancer 31A(13-14): 2347-2353, December 1995.
6. Hager E.D.: "Unkonventionelle Tumortherapie-Status quo: Aktive Immunotherapie und Biomodulation." Forsch Komplementaermed 1994; 1 (suppl. 1): 18-25.
7. Horsman MR, Chaplin DJ, Brown DM: Radiosensitization by nicotinamide in vivo: a greater enhancement oftumor damage compared to that of normal tissues. Radiat Res 109:479-489, 1987.
8. Horsman MI, Chaplin DJ, and Overgaard J: The use of blood flow modifiers to improve the treatment response of solid tumors. Radiother Oncol 20(Suppl): 47-52, 199 1.
9. Joachim Fluhrer, “Patient Management - Supportive Cancer Therapy “, Journal of the Australasian College of Nutritional & Environmental Medicine, Vol. 14, No. 2, November 1995, pages 5-8 + 20.
10. Kim JH, et. al.- Use of vitamins as adjunct to conventional cancer therapy. In Prasad KN, et al (eds): Nutrients in Cancer Prevention and Treatment. Totowa: Humana Press, 1995.
11. Kjellen E, et al. A therapeutic benefit from combining normobaric carbogen or oxygen with nicotinamide in fractional X-ray treatments. Radiother Oncol 22(2): 81-91, October 1991.
12. Lissoni P, et al. Melatonin as a new possible anti-inflammatory agent. J Biol Regul Homeeost Agents 11(4): 157-159, October/December 1997.
13. Myers CE, et al-. Effect of tocopherol and selenium on defenses against reactive oxygen species and their effects on radiation sensitivity. Ann NT Acad Sci 393:419-425,1982.
14. Okunieff P, et al-. Interactions between ascorbic acid and the radiation of bone marrow, skin, and tumor. Am J Clin Nutr 51(12): 128 IS- 1283S, December 1991.
15. Prasad KN: Vitamin E induces differentiation and growth inhibition, and enhances efficacy oftherapeutic agents on cancer ccfls. In QuiUin P, Williams RM (eds): Adjuvant Nutrition in Cancer Treatment. 1992 Symposium Proceedings, pp. 235-252. Arlington Hgts: Cancer Treatment Research Foundation, 1993.
16. RheeYH, et al-. Inhibition of mutagenesis and transformation by root extracts of Panax ginseng in vitro. Planta Medica 57:125-128, 1991.
17. Ripamonti C, et al-. A randomized, controlled clinical trial to evaluate the effects of zinc sulfate on cancer patients with taste alterations caused by head and neck irradiation. Cancer, 82:1938-1945, 1998.
18. Stahelin HB: Critical reappraisal of vitamins and trace minerals in nutritional support of cancer patients. Supportive Care in Cancerl (6): 295-297, November 1993.
19. Tallberg Th., Tykka H., Haltunen P., et al.: "Cancer Immunity. The effect in cancer immunotherapy of polymerized autologous tumor tissue and supportive measures." Scand. J. Clin. Lab. Invest. 1979; 39:1-35.
20. Treskunov K.A. in the book of “Memoirs of Phytotherapist” – 12003, Moscow, pp205—208.
21. Wadleigh RG, et al-. Vitamin E in the treatment of chemotherapy-induced mucositis. Am J Med92 (5): 481-484, May 1992.
22. Wadleigh RG, et al. Vitmiin E in the treatment of chemotherapy-induced mucositis. AmjMed92 (5): 481-484, May 1992.
23. Histopathological study of the mode of action of therapy with Aloe Vera. Cancer, 6:690-698, 1953.
24. White LB: Recovering from surgery. Health & Nutrition Breakthroughs 2(8): 30-33, August 1998.
25. Wood U- Possible prevention of adriamycin-induced alopeia by tocopherol. New England Journal of Medicine 312(16): 1060, April 1985.
26. Wright TV: Surgery? Quicker, stronger, less painful healing. Nutrition & Healing 12, January 1996.
27. Yalkut S.I. at al.: “Potential of phytotherapy in the treatment of digestive tract cancer patients” Oncology 2000, 2: 135-140.
28. Yoshida S, et al-. Compression-induced brain edema: modification by prior depletion and supplementation of vitamin E. Neurology 33(2): 166-172, February 1993.
K.A.Treskunov, O.K. Treskunova,
B.A.Komarov, A.V.Goroshetchenko, I.I. Pilipenko, V.I.Glebov, D.M.Martirosyan*.
Hospital at Russian Academy of Science, Chernogolovka, Russia;
Ecology and Health Association, Moscow, Russia;
Scientific Medical Center, Moscow State University, Moscow, Russia;
Health and Long – Living Center, Russia;
D&A Inc., Richardson TX, USA.
Hospital at Russian Academy of Science, Chernogolovka, Russia;
Ecology and Health Association, Moscow, Russia;
Scientific Medical Center, Moscow State University, Moscow, Russia;
Health and Long – Living Center, Russia;
D&A Inc., Richardson TX, USA.
Summary
On the base biomedical properties and computerized analyses of traditional and non-traditional plants we determine the effectiveness of action of medical plants to the symptoms, syndromes and different kind of oncological diseases in general. The best results in the treatment of oncological patients we reached with usage of necessarily surgery, with accompany chemotherapy and radiation therapy and with combination of phytotherapy. Treatment by this schema with usage of our new formulas enhanced the average of survivals the first year after treatment from 39% (official data of Russian Health Ministry) to 90%, in our case. More than 50% of our patient treated by this way lived more than 5 years. According to our new approach cancer is chronic disease, with weakness of immune system. So, it should be treated as a chronic disease with monitoring of immune system. To be sure that recurrence of malignant is not appears any more it was created special formula, which can be used during the whole lifetime.
The aim of cancer therapy is the destruction of the tumor and to preserve function and lengthen survival time. The main therapies are surgery, chemotherapy and radiotherapy. However, they may negatively impact quality of life. Because only maximum dosages can eliminate all malignant cells and cytotoxic substances not only damage the tumor cells, they also affect all other bodily systems. Medical Plants can help minimize side effect of conventional treatment. Recent studies demonstrate that, even after maximum therapy (surgery, radiation, and chemotherapy) still about 0.1% of rest tumor cells have survived (Joachim Fluhrer 1995). Only the immune system is then capable of achieving a cure. Usually immune system can destroy these remaining malignant cells, but the tumor-destructive therapies have damaged the immune system quite extensively. Therefore a high risk of recurrence and metastases will exist. Phytotherapy can be used to optimize the endocrinological therapy and stimulate the immune system. During phytotherapy a supportive therapy for liver function and the micronutrient balance is essential. Phytotherapy can be employed as an effective method in the treatment of digestive tract cancer allowing us to individualize therapy accordind to immunologic, endocrine and metabolic characteristics of the patients (S.I.Yalkut, et al.-2000). All immunologic effective substances need to be considered such as the vitamins, phytochemicals, such as
*Corresponding author: Dr. Danik M. Martirosyan, D&A Inc., Richardson, TX, USA, E-mail: danikm@sbcglobal.net
anthocyanosides, phenolic acids, flavonoids, coumarins, poly-acetylenes and carotenoids. This article explores the role of Phytotherapy for improving the quality of life, and perhaps survival time, of oncological patients.
Materials and Methods
For the treatment of oncological diseases we used medical plants by the fallowing way:
Dry botanical collections (Species);
Could infusions (Infusum);
Hot infusions (Infusum);
Decoctions (Decoctum);
Unguents (Unguentum);
Pills from dry herbs with special extenders (Tabulettae);
Phytochitodeses made on the base of chitosan and botanical collections.
All this materials was made by special methods described by Dr. Treskunov K.A. in the book of “Memoirs of Phytotherapist” – 12003, Moscow, pp 205—208.
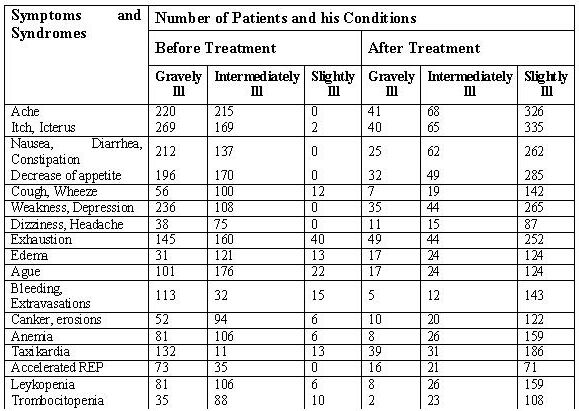
Treatment was provided with monitoring of syndromes, symptoms and immune system. Monitoring of immune system we reach by investigations of formal elements of blood system, in particularly trombocytes, leucocytes, erythrocytes and CEO. Monitoring of syndromes and symptoms was provided by investigations of Ache, Itch, Icterus, Nausea, Diarrhea, Constipation, Decrease of appetite, Cough, Wheeze, Exhaustion, Weakness, Depression, Dizziness, Headache, Edema, Ague, Bleeding, Extravasations, Canker, erosions and Anemia.
First step of treatment of oncological patients with herbal plants we start 2-3 days before surgery, chemotherapy and radiation. Our formula (number 02), which is used in the step 1 contain Chamomile, Goose Grass, Mint, Tutsan and Milfoil. Patients can used that as a pill or as a capsule. There are not side effects from those and at present time they are proved from Russian Ministry of Health Ministry. This formula mainly we using for the stimulation of immune system and to preventing the side effects of chemical and radiation therapy.
Second step is prevent and treatment of the side effects of chemotherapy and radiation. After conventional treatments often have been observed anemia, leykopenia, trombocitopenia. In this step we are using formula number 05, which contain more than 20 plants. Patients using this formula as a tablets 3-4 times a day within 10-12 days until immune and blood system renewal.
Third step is usage of formula number 01. This one oncological patient have to use during the hole life time, without any brake more than 1 month, to be sure that recurrence is not appears any more.
Results.
Table 1. The effect of phytotherapy to the symptoms and syndromes of patients with oncological diseases.
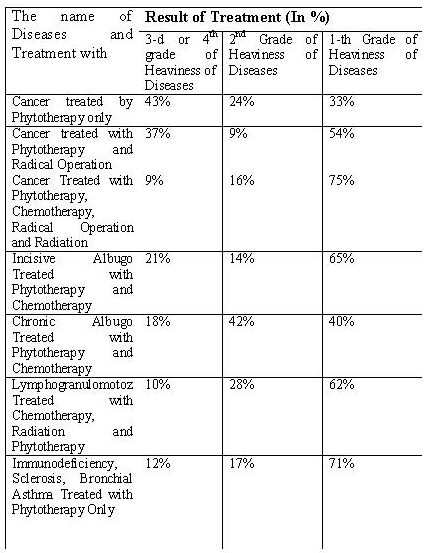
Table 2. The Effectiveness of Phytotherapy with Conventional
Treatment in the Case of Oncological and other Heavy Diseases.
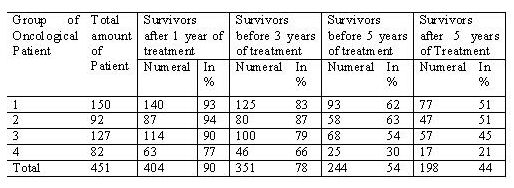
It was investigated 4 groups of oncological patients. First group content 150 patient which is 33% from total amount of oncological patient to whom was provided phytotherapy with surgery, chemotherapy and (or) Radiation. The second group composed of 92 people, which is 20% of total patients. They get surgery additional to the phytotherapy.
The third grope was 127 patient (28% from total amount) who get phytotherapy, chemotherapy and (or) radiation, without surgery. Forth group composed of 82 patients, which is 19% of total amount. They were treated with only phytotherapy.
Table 3. The Effect of Phytotherapy with and without Conventional Healing to the survival of Oncological Patients
Discussion.
Our data shown that the treatment with phytotherapy jointly with surgery, radiation and chemotherapy provide the best results (group 1 and group 2). It is interesting that 21% survivors of oncological patients treated only with phytotherapy, without any conventional healing live more than 5 years. It was shown also that in the case of combination of surgery, chemotherapy, and radiation with phytotherapy there is no complication, which is usually having a place without herbal healing. We find out also, that the usage of our formulas as a tea lifelong prevents beginning of recurrences.
It is well known, that each year in Russia apiaries more than 400 000 oncological patients. From thous 39% only usually live more than 1 year. Thus we contributed a new approach for treatment of oncological diseases. The new approach considering condition of immune system of patient before and after conventional cure. It is known that Immune system become a week after radiation and chemotherapy.
As a pioneer we receive a authentic statistics which proved effectiveness of phytotherapy in general and effectiveness of each herbal plant in particular, which we using in depends of syndromes and symptoms, illness, etiology and pathogenesis. On the base of computerized analyses we find out the effectiveness’s of action of medical plants to the symptoms, syndromes and diseases. Thus we determine that the most effective among the investigated plants as an anesthetic is “air bolotniy”, then “shalfey lekarstvenniy”, and tarragon at cetera. This is very important because in the case of oncological diseases usually appears strong pain, which is only you can decrease with anesthetics. Furthermore we find out that in the case of weight lose the best medical plant are “xvoshch polevoy”, nettle, coltsfoot, mint and chamomile. This allows as composing most effective phyto collection for each individual patient. With the usage of phytotherapy in our case disappears or vastly decreases pain, renew of leucocytes (78%) vomit (75%), thrombocytes (80%), hemoglobin – 65%, renew weight of body (70%), disappears depression (77%) and weakness (77%). The usage of chemotherapy and radiation jointly with phytotherapy prevents the development of chemical or X-ray illness.
Numerous published protocols confirm the importance of nutrition’s and herbal therapy in speeding post-surgical healing and reducing pain, swelling, and complications (Wright TV, 1996; White LB, 1998). Supplement protocols begun 1-2 weeks prior and continuing 3-4 weeks post-surgery-commonly include a daily intake of Vitamin C (3,000 mg), Bioflavonoids (1,500 mg), Vitamin E (400 IU), Vitamin A (25,000 IU), and Zinc (30 mg). Proteolytic enzymes--well researched in cancer treatment are particularly helpful in reducing swelling and enhancing wound healing.
Our results confirm that the usage of phytotherapy in our case vastly decreases pain, weakness and anemia but its also lead to the renew of leucocytes (78%), thrombocytes (80%), hemoglobin – 65%. This is can prove our hypothesis, that phytotherapy can be directly involved in the renewal of weak immune system of oncological patient.
There is a strong connection between tumor genesis and immunological “weakness”. With the knowledge we have today about this connection, no oncological therapy should be done without immunological control. After the diagnosis of cancer, the damaged cellular defense mechanism has to be treated and restored as early as possible. Consequent immune monitoring and specific immune modulation increases the chances of successful therapy. Many substances with immunological effect have a high degree of importance in the supportive cancer therapy of any cancer patient. It is well known that macrophages, NK-cells, cytotoxic cells and helper cells can attack malignant cells and destroy them (Hager E.D. 1994). At the time of diagnosis, and even before, one usually finds a very low cellular immunity. Tumor-associated antibodies produce immunocomplexes, together with the corresponding antigens. Above a certain concentration, macrophages are not able to destroy those immunocomplexes any more (Joachim Fluhrer, 1995). These complexes will then build a barrier around the tumor and therefore prevent an active immunological reaction against tumor cells. In higher concentration, circulating immunocomplexes block the function of macrophages and so paralyze an important defense mechanism. A healthy defense and immune system can identify and destroy cancerogenic substances and disease will not ensue. If the limit of the compensatory ability of the immune system is reached, or if there is a cellular immunodeficiency, then penetration of the cancerogenic substances into the basal membrane or the cell membrane can occur (Tullberg Th., 1979). Interaction with nuclear DNA will lead to the formation of oncogenes and oncogenic cells. Tumor antigens can stimulate the production of specific antibodies, which are directed against specific cell structures. If the immune system is still intact the 'malignant' process can still be interrupted and total restoration is possible. If the cellular immune system is too weak, uncontrolled growth of tumor cells can occur, either encapsulated or invasive. The encapsulated tumor can be removed surgically and a cure is possible. If the cancer has invaded the blood vessels or lymphatic system, then malignant cells have become systemic. Even then the immune system has the possibility to identify and destroy the malignant cells and prevent the progression of the disease (Joachim Fluhrer, 1995. In our case phytotherapy at this stage is still effective (21%), but it is mach better if it is provided with surgery and other forms of conventional treatment (51%). If treatment of cancer with phytotherapy jointly surgery is missed, then the 'malignancy' has escaped the control of the immune system and will lead to the death of the patient.
Monitoring the immune system at the time of diagnosis and then regularly afterwards is of extreme importance. In the first 2 years following the diagnosis and treatment of cancer, a 6-weekly monitoring of the immune status should be done, especially if immune-modulator therapies are being used. After stabilization less frequent monitoring is necessary. It should be monitored the fallowing cells of immune system: T-Lymphocytes, suppressor cells, helper cells, Macrophages, B-lymphocytes, leucocytes, thrombocytes, hemoglobin.
Immune Modulation in Cancer Therapy can be provided as well as with phytotherapy and with Phytochemicals, including Quercetin and Rutin, Micronutrients, such as Zinc, Magnesium, Selenium, Lithium, with vitamins such as Vitamin A, Beta-Carotene, Vitamin C, Vitamins B2, B6, B12 and Folic Acid.
In the case of Immune therapy may activate sub clinical infections (e.g. silent dental abscesses, ostitis, impacted wisdom teeth, etc.) and therefore enhance the biological stress. This may lead to a worsening of the immunological status. Usually herbal therapy has not side effect, so we suggesting provide phytotherapy with monitoring immune system. Only after effective therapy will the cellular immune defense rise again. To enhance the efficacy of Radiation Therapy we provided phytotherapy with the fallowing plants:
We believed that these plants supplied the body with necessary phytochemicals and nutrients also. Usually, enhancing the efficacy of Radiation Therapy provided with niacin, Anti-oxidants, Vitamin C, and Vitamin E. Oxygen is a potent radiation sensitizer. Hypoxic (oxygen-deficient) tumors are resistant to radiation. Natural agents that increase blood flow may improve radiation response by delivering oxygen to tumors, thereby increasing tumor vulnerability to radiation. Niacin (500 mg to 6,000 mg of nicotinamide) is an effective radio-sensitizer, while producing little or no radio-sensitization of normal tissues.13-17 however, prolonged intake of larger doses of niacin may lead to liver damage. Inositol hexaniacinate may be a preferable form. It is safer, well tolerated, and effectively improves circulation and oxygenation.18 Radiotherapies are believed to achieve their cytotoxic effect by generating free radical-mediated DNA damage to the tumor. The use of anti-oxidants during radiation therapy appears counter-indicated in theory. However, research published over the past 30 years supports the adjunctive use of anti-oxidant nutrients, with improved radiation treatment results and protection of healthy tissues (Cheraskin E, et al-1968; Funegard U, et al., 1995; Stahelin HB, 1993; Wood U, 1985; Wadleigh RG, et al-. 1992; Lissoni P, et al. 1997).
Vitamin C Increases tolerance to radiation therapy without reducing tumor control (Okunieff P, et al-1991). Vitamin E is also an effective adjunct to radiation (Prasad KN, 1993; Myers C.E., et al.1982). It protects against brain edema (Yoshida S, et al-.1992), a side effect of brain irradiation. Vitamin E intake (800 IU/day) can be divided between d-alpha tocopheryl succinate, which does not act as an anti-oxidant and provides some anti-tumor effects, and a mixed tocopherol product.
Side effects of Radiation Therapy commonly associated with brain irradiation include loss of hair, skin burn, loss of taste, and pervasive fatigue. Radiation damage to salivary glands and taste buds can result in a dry, irritated mouth and loss of taste perception. This can decrease the desire and ability to eat, seriously impacting nutritional status. Post RT healing can be provided with zinc, flaxseeds, Topical vitamin E, Aloe Vera and Ginseng. Zinc supplementation (15-45 mg, as lozenges or liquid zinc sulfate) at onset of loss of taste can restore taste perception (Ripamonti C, et al.1998). Supplementation with antioxidant nutrients--from 14 days prior through 12 days post-RT---can reduce damage to salivary glands (Funegard U, et al., 1995) Water extracts of flaxseed can provide relief of dry, irritated mouth and replace lost saliva (Andersson G, et al, 1995). Topical vitamin E is effective in oral mucositis (Wadleigh RG, et al, 1992). Topical application of 100% concentrate of Aloe Vera after daily RT treatments can be helpful for radiodermatitis. Vitamin E supplementation (1,600 IU/day), begun one week prior to RT, allowed more than half the patients to keep their hair, and dramatically reduced fatigue. Ginseng is best restricted to recuperation following RT (15-30 days post-RT), because it stimulates DNA rep
Further studies are needed in the specific effect on cancer cells. From our investigations we can make the fallowing conclusions:
1. On the base biomedical properties and computerized analyses of traditional and non-traditional plants we find out the effectiveness of action of medical plants to the symptoms, syndromes and different kind of oncological diseases.
2. It was created new formulas, which are enhancing the damaged cellular defense mechanism of oncological patients. They prevent the beginning of side effects of chemotherapy and radiation therapy and healing the side effects of conventional therapy. There are not side effects from these formulas, they are cast effective and at present time they are proved from Russian Ministry of Health Ministry.
3. The best results in the treatment of oncological patients we reached with usage of necessarily surgery, with accompany chemotherapy and radiation therapy and with combination of phytotherapy. Treatment by this schema with usage of our new formulas enhanced the average of survivals the first year after treatment from 39% (official data of Russian Health Ministry) to 90%, in our case. More than 50% of our patient treated by this way lived more than 5 years.
4. According to our new approach cancer is chronic disease, with weakness of immune system. So, it should be treated as a chronic disease with monitoring of immune system each 6 month. To be sure that recurrence of malignant is not appears any more it was created special formula, which can be used during the whole lifetime.
References:
1. Andersson G, et. al. Comparison of the effect of the
linseed extract salinum and a methylcellulose preparation on the symptoms
of dry mouth. Gerodantoloffl 12(l): 12-17, July 1995. 2. Brown JM, et al. Structure-activity relationships for turnour radio-sensitization by analogues of nicotinamide and benzamide. Int J Radiat Biol 59(3): 739-748, March 1991.
3. Cheraskin E, et al. Effect of diet upon radiation response in cervical carcinoma of the uterus: a preliminary report. Acta Cytol 12(6): 433, November/December 1968.
4. Funegard U, et al. Can alpha-tocopherof and beta-carotene supplementation reduce adverse radiation effects on salivary glands? Europ J Cancer 31A(13-14): 2347-2353, December 1995.
5. Funegard U, et al. Can alpha-tocopherol and beta-carotene supplementation reduce adverse radiation effects on salivary glands? Europ J Cancer 31A(13-14): 2347-2353, December 1995.
6. Hager E.D.: "Unkonventionelle Tumortherapie-Status quo: Aktive Immunotherapie und Biomodulation." Forsch Komplementaermed 1994; 1 (suppl. 1): 18-25.
7. Horsman MR, Chaplin DJ, Brown DM: Radiosensitization by nicotinamide in vivo: a greater enhancement oftumor damage compared to that of normal tissues. Radiat Res 109:479-489, 1987.
8. Horsman MI, Chaplin DJ, and Overgaard J: The use of blood flow modifiers to improve the treatment response of solid tumors. Radiother Oncol 20(Suppl): 47-52, 199 1.
9. Joachim Fluhrer, “Patient Management - Supportive Cancer Therapy “, Journal of the Australasian College of Nutritional & Environmental Medicine, Vol. 14, No. 2, November 1995, pages 5-8 + 20.
10. Kim JH, et. al.- Use of vitamins as adjunct to conventional cancer therapy. In Prasad KN, et al (eds): Nutrients in Cancer Prevention and Treatment. Totowa: Humana Press, 1995.
11. Kjellen E, et al. A therapeutic benefit from combining normobaric carbogen or oxygen with nicotinamide in fractional X-ray treatments. Radiother Oncol 22(2): 81-91, October 1991.
12. Lissoni P, et al. Melatonin as a new possible anti-inflammatory agent. J Biol Regul Homeeost Agents 11(4): 157-159, October/December 1997.
13. Myers CE, et al-. Effect of tocopherol and selenium on defenses against reactive oxygen species and their effects on radiation sensitivity. Ann NT Acad Sci 393:419-425,1982.
14. Okunieff P, et al-. Interactions between ascorbic acid and the radiation of bone marrow, skin, and tumor. Am J Clin Nutr 51(12): 128 IS- 1283S, December 1991.
15. Prasad KN: Vitamin E induces differentiation and growth inhibition, and enhances efficacy oftherapeutic agents on cancer ccfls. In QuiUin P, Williams RM (eds): Adjuvant Nutrition in Cancer Treatment. 1992 Symposium Proceedings, pp. 235-252. Arlington Hgts: Cancer Treatment Research Foundation, 1993.
16. RheeYH, et al-. Inhibition of mutagenesis and transformation by root extracts of Panax ginseng in vitro. Planta Medica 57:125-128, 1991.
17. Ripamonti C, et al-. A randomized, controlled clinical trial to evaluate the effects of zinc sulfate on cancer patients with taste alterations caused by head and neck irradiation. Cancer, 82:1938-1945, 1998.
18. Stahelin HB: Critical reappraisal of vitamins and trace minerals in nutritional support of cancer patients. Supportive Care in Cancerl (6): 295-297, November 1993.
19. Tallberg Th., Tykka H., Haltunen P., et al.: "Cancer Immunity. The effect in cancer immunotherapy of polymerized autologous tumor tissue and supportive measures." Scand. J. Clin. Lab. Invest. 1979; 39:1-35.
20. Treskunov K.A. in the book of “Memoirs of Phytotherapist” – 12003, Moscow, pp205—208.
21. Wadleigh RG, et al-. Vitamin E in the treatment of chemotherapy-induced mucositis. Am J Med92 (5): 481-484, May 1992.
22. Wadleigh RG, et al. Vitmiin E in the treatment of chemotherapy-induced mucositis. AmjMed92 (5): 481-484, May 1992.
23. Histopathological study of the mode of action of therapy with Aloe Vera. Cancer, 6:690-698, 1953.
24. White LB: Recovering from surgery. Health & Nutrition Breakthroughs 2(8): 30-33, August 1998.
25. Wood U- Possible prevention of adriamycin-induced alopeia by tocopherol. New England Journal of Medicine 312(16): 1060, April 1985.
26. Wright TV: Surgery? Quicker, stronger, less painful healing. Nutrition & Healing 12, January 1996.
27. Yalkut S.I. at al.: “Potential of phytotherapy in the treatment of digestive tract cancer patients” Oncology 2000, 2: 135-140.
28. Yoshida S, et al-. Compression-induced brain edema: modification by prior depletion and supplementation of vitamin E. Neurology 33(2): 166-172, February 1993.
К списку докладов на конференции
.
За разъяснениями, а так же с предложениями, оценками и.т.д. можно обратиться по этому адресу: